ACUTE BILIARY PANCREATITIS
Posted on 2023-07-27 03:47:46 by SathishThis is one of the complications of gall stone disease. Once the gall stone migrates down to the bile duct it can cause pain, jaundice and fever. Extension of this problem is that the stone can block the pancreatic duct at the ampulla of Vater and leads to the development of pancreatitis.
The obstruction of the pancreatic duct by the bile duct stones leads to increase in the pancreatic ductal pressure. The increased pancreatic duct pressure causes regurgitation of bile and pancreatic juice into the pancreatic parenchyma. This leads to pancreatic tissue damage. This condition is known as acute biliary pancreatitis.
The patient with acute biliary pancreatitis will present with severe pain abdomen associated with vomiting. Pain will be in the upper abdomen and radiates to back. There will be abdominal distension and vomiting. Severe form of acute pancreatitis can lead to involvement of other organs like kidney and lung damage and may end up with malfunctioning of these organs. In acute biliary pancreatitis patients will typically appear with significant abdominal pain and vomiting. Upper abdominal pain radiates to back. In Severe Acute Pancreatitis, it can damage other organs such as the kidneys and the lungs and may eventually leads to malfunction of these organs.
The diagnosis of acute biliary pancreatitis is suspected by the clinical presentation of acute abdominal pain with jaundice. This condition more commonly seen in persons diagnosed to have gall stone disease immediately after delivery.
So, any patient with gall stone disease in the younger age group, waiting for conception should undergo gall bladder removal surgery electively even in the absence of symptoms to prevent the gall stone induced complications after delivery.
The diagnosis of biliary pancreatitis is made by ultrasonography of abdomen, liver function test along with serum amylase and lipase estimation. Increased serum amylase and lipase with increase in serum bilirubin and liver enzymes along with presence of stones in the gall bladder by ultrasonography of the abdomen will nearly confirm the diagnosis of acute biliary pancreatitis.
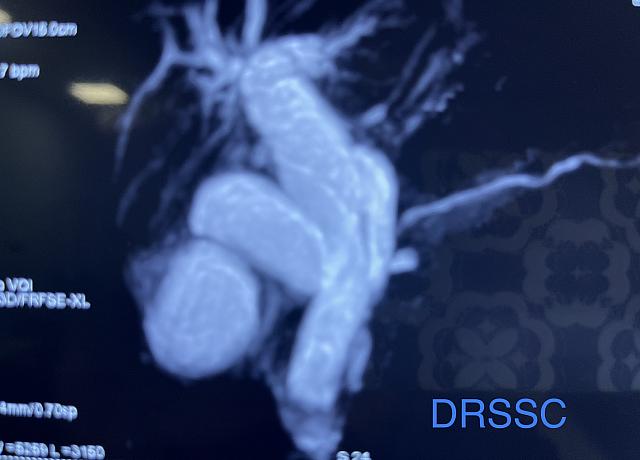
Sometimes the migrated stone from the gall bladder into the common bile duct may pass out in to the duodenum through ampulla spontaneously. So, in patient with biliary pancreatitis, MRCP test become mandatory to assess the bile duct which helps to plan further treatment.
Computerized tomography of the abdomen done with intravenous contrast will assess the severity of the pancreatitis. The absence of contrast flow into the pancreatic tissue suggests the possibility of severe pancreatic damage (pancreatic necrosis).
The treatment of acute biliary pancreatitis is complex. The treatment plans must include the following:
First is to treat the pancreatitis and stabilize the patient. This is usually done with admitting the patient, keeping the patient with nil by oral, intravenous fluids, pain killers, antacids, antibiotics in case of suspected infection along with slow intravenous infusion of special hormone called somatostatin or its analogue octreotide. This is a hormone supposed to reduce the severity of acute pancreatitis.
Clinical assessment is done for the improvement of symptoms. Once the patient get stabilized, next is to treat the bile duct stones. The presence of bile duct stones is confirmed with MRCP. The bile duct stones are treated with ERCP and stone extraction. The idea of doing ERCP and stone extraction is to prevent the further attack of acute biliary pancreatitis.
One important point to be remembered is that, resolving time of severe acute pancreatitis is about three to six months. So, by doing ERCP and stone removal from the bile duct will prevent the further attack of acute biliary pancreatitis but may not have impact on the existing pancreatitis.
After stone extraction from the bile duct, a stent is placed and the clinical improvement of the patient is observed. If patient is recovering from pancreatitis, then the gall bladder removal operation is considered. But in case of any complications due to pancreatitis, the treatment should be considered first to the complications of pancreatitis. The complications of pancreatitis are infection, necrosis, fluid formation around the pancreas, pseudocyst formation and other organ failures. Just a small number of individuals may experience these problems, which necessitate special care and constant monitoring.
Once the patient is recovering smoothly from the acute biliary pancreatitis then the gall bladder removal operation is considered. This procedure is usually done by laparoscopy. There may be some technical difficulties in these patients like adhesions and difficult dissection of Calot’s triangle. In case of any difficulty open surgery will be the option.
It has to be remembered that even after ERCP with bile duct stone removal followed by laparoscopic or open cholecystectomy, problems related to the first biliary pancreatitis attack, such as pancreatic necrosis, infection of pancreatic necrosis, or pseudocyst development, might still occur within six months.